
Physicians spend an average of 3.1 hours daily on EHR documentation. That number comes from a 2023 AMA Physician Burnout Study. It is not a rounding error. That is more time on software than on patients.
Most EHR platform were not built for the people using them. They were built for compliance checkboxes, billing workflows and vendor profit margins. The result is a system that fights your team instead of helping them.
Custom EHR software development fixes that from the ground up. It builds around your clinical reality. It connects your departments, your specialties and your compliance requirements in one place.
This guide covers everything your team needs to make the right decision. What EHR development actually means. What it costs. How long it takes and what separates strong development partners from weak ones.
If you are evaluating custom EHR development in 2026, this is the guide you need.
What Is EHR Software Development And Why Are Generic Solutions Failing ?
EHR software development is the process of designing, building and deploying a digital system that manages patient health records across care settings. That is the direct answer.
But the fuller picture matters more for decision-makers in healthcare organizations.
An EHR is not a database. It is a clinical operating system. It connects patient demographics, lab results, imaging data, medications, billing records and provider communication in one platform.
What Is the Difference Between EHR and EMR?
This distinction trips up many buyers, so here is the short version.
An EMR is a digital version of a paper chart. It stays inside one practice. One provider sees it. It does not travel with the patient.
An EHR is built for interoperability. It follows the patient across providers, hospitals, labs and specialists. It is designed to share data, not just store it.
For most healthcare organizations in 2026, EHR is the right target. EMR-only systems create data silos. Silos create care gaps. Care gaps have real consequences.
Why Are Generic EHR Platforms Failing Clinical Teams?
Off-the-shelf EHR platforms like Epic and Cerner serve a broad market. They were built for the median hospital, not your hospital.
A 2024 KLAS Research report found that 67% of clinicians say their EHR slows them down rather than helping them. That number has not improved in three years.
The reasons are consistent across organizations. Inflexible workflow templates. Feature sets built for billing over care. Integration walls between departments. And upgrade cycles that require expensive consultant projects.
Custom EHR software development solves these issues at the root. It builds around your specific workflows, not a generic template someone else chose years ago.
The 6 Types of EHR Systems — Which One Does Your Organization Actually Need?

Not all EHR systems solve the same problem. Choosing the wrong type creates integration headaches that last for years. Here are the six categories that matter in 2026.
1. Ambulatory EHR
Designed for outpatient settings. This includes physician practices, specialist clinics, and urgent care centers. Ambulatory EHRs focus on appointment scheduling, e-prescribing and chronic disease management. They are lighter than hospital systems but must connect to lab and pharmacy networks.
2. Inpatient EHR
Built for hospitals and acute care settings. These manage complex, multi-department workflows. Inpatient EHRs handle nursing notes, surgical records, medication administration, and real-time monitoring data. They are larger, more complex, and take longer to implement.
3. Specialty EHR
Tailored to specific clinical disciplines. Mental health, dentistry, ophthalmology, oncology, and cardiology each have unique documentation needs. A mental health EHR needs therapy note templates, SAMHSA compliance controls, and crisis intervention tracking. A generic EHR handles none of that well.
4. Post-Acute EHR
Designed for long-term care, skilled nursing facilities, home health agencies, and rehabilitation centers. These systems manage care plans across weeks or months. They connect to Medicare and Medicaid billing systems and support complex coordination workflows.
5. Cloud-Based EHR
Hosted on secure cloud infrastructure. Access comes through a browser or app, not local servers. Cloud-based EHRs reduce upfront infrastructure cost. They support automatic updates and better scalability. AWS and Azure healthcare-compliant environments are the most common hosting choices in 2026.
6. Modular EHR
Built as a core platform with add-on modules. Organizations start with the essentials and expand over time. This approach works well for organizations with phased budgets or those migrating from a legacy system. It reduces initial risk while preserving long-term flexibility.
Why Healthcare Organizations Are Moving to Custom EHR in 2025-26?
The global EHR market is projected to reach $40.5 billion by 2030, according to Grand View Research. That growth is not happening because hospitals are satisfied with existing platforms.
It is happening because organizations are replacing systems that no longer serve them.
Three Forces Driving Custom EHR Adoption Right Now
The first is the 2024 ONC Information Blocking Rule. Effective January 2024, healthcare providers are legally prohibited from blocking the flow of electronic health information. EHR platforms with closed APIs now create direct compliance liability.
The second is TEFCA. The Trusted Exchange Framework and Common Agreement establishes a national framework for health information exchange. Organizations that cannot connect to qualified health information networks will be shut out of coordinated care models.
The third is AI integration. Hospital systems that want ambient documentation, predictive analytics and AI-assisted clinical decision support cannot bolt these features onto legacy EHRs. They need systems built to support AI from day one.
What This Means for Healthcare Decision-Makers
If your current EHR does not support FHIR R4 APIs and open data exchange, you are already behind the compliance curve. Custom EHR development gives organizations the architecture to meet 2024 and 2025 regulatory requirements. No workarounds. No third-party compliance patches.
Build vs. Buy vs. Customize : The Decision Framework Every Healthcare CTO Needs
This is the question every healthcare technology leader faces. The right answer depends on three things: workflow complexity, compliance exposure and five-year budget modeling.
Here is a framework that cuts through the noise.
| Factor | Buy (Off-the-Shelf) | Customize (Extend Existing) | Build (Custom Development) |
|---|---|---|---|
| Time to Deploy | 3 to 6 months | 6 to 12 months | 9 to 18 months |
| Upfront Cost | $50K to $500K licensing | $100K to $800K | $150K to $2M+ |
| Workflow Fit | Low — built for the median | Medium — limited by base system | High — built for your workflows |
| AI Integration | Limited or locked | Partial — depends on vendor API | Full — designed from day one |
| FHIR R4 Compliance | Varies by vendor | Partial | Fully controllable |
| Long-Term Cost | High — licensing scales with providers | Medium — hybrid maintenance model | Lower — you own the system |
| Data Ownership | Vendor controls your data | Shared control | Full ownership from day one |
| ONC Info Blocking Rule | Risky with closed APIs | Depends on vendor | Compliant by design |
| Best For | Small practices, tight budgets | Mid-size orgs, legacy migration | Complex care settings, growth plans |
How to Use This Framework
Start with workflow complexity. If your care model is standard primary care with no specialty requirements, buying makes sense. If you run a multi-specialty system, a mental health network, or a post-acute facility, customization or custom development is almost always the right call.
Then look at your five-year budget. Licensing costs for large EHR platforms scale aggressively with provider count. At 500 or more providers, annual licensing often exceeds the amortized cost of a custom system. Finally, consider data ownership. In a custom-built system, your patient data belongs to your organization. In a vendor-hosted platform, data portability is often contractually restricted.
Must-Have Features in Custom EHR Software Development
A custom EHR is only as strong as the features inside it. This list reflects what clinical organizations actually need in 2026, not what vendors were building in 2019.
Core Clinical Features
- Patient demographics and unified health record across all encounters
- Clinical documentation templates built for your specific specialty
- Medication management with drug interaction alerts and e-prescribing
- Lab and imaging order management with direct system integration
- CPOE (Computerized Physician Order Entry) with clinical decision support
- Problem list, allergy tracking, and immunization history
AI and Automation Features
- Ambient clinical documentation using LLM-powered voice transcription
- AI medical scribe that converts encounters into structured SOAP notes
- Predictive analytics for patient risk scoring and readmission prevention
- AI-assisted clinical decision support for diagnosis and treatment pathways
- Natural language processing for extracting data from unstructured notes
Interoperability and Integration Features
- FHIR R4 API layer for real-time data exchange with external systems
- HL7 v2 and v3 messaging for legacy system compatibility
- SMART on FHIR app framework for third-party clinical tools
- Patient portal with secure messaging and health record access
- Telemedicine integration with video consultation and remote monitoring
Administrative and Billing Features
- Automated ICD-10 and CPT coding assistance to reduce billing errors
- Revenue cycle management (RCM) module with claims processing
- Insurance eligibility verification at point of scheduling
- Appointment scheduling with automated reminders and no-show tracking
- Audit trail and access logging for HIPAA compliance
Specialty-Specific Features Worth Considering
- Mental health: therapy note templates, crisis flags, SAMHSA compliance controls
- Oncology: treatment protocol tracking, chemotherapy dosing, tumor registry
- Cardiology: ECG integration, hemodynamic data, cardiac event logging
- Pediatrics: growth chart tracking, vaccine schedule management, parental access controls
- Home health: mobile-first interface, offline mode, GPS-enabled field documentation
The Complete Compliance Blueprint for EHR Development
Healthcare compliance is not a checklist you add at the end. It is an architecture decision that shapes every line of code your development team writes.
Here is what the compliance landscape looks like in 2026.
HIPAA and HITECH Requirements
The Health Insurance Portability and Accountability Act requires any system handling Protected Health Information to implement three categories of safeguards: administrative, physical, and technical.
For an EHR system, this means end-to-end encryption for all data in transit and at rest. Role-based access controls that limit PHI access to authorized users only. Audit trails that log every data access and modification event. Automatic session timeouts and multi-factor authentication across all access points.
HITECH extended HIPAA enforcement to business associates. Any third-party vendor, API, or cloud service that touches PHI must be HIPAA compliant. This includes your cloud hosting provider and any integrated lab or pharmacy management system.
The 2024 ONC Information Blocking Rule
Effective January 2024, healthcare providers are legally prohibited from blocking the sharing of electronic health information. This applies to providers, health IT developers, and health information networks alike.
Non-compliance carries civil monetary penalties of up to $1 million per violation. Any EHR system with a closed data architecture now represents a direct regulatory liability for your organization.
A properly built custom EHR uses open FHIR R4 APIs by design. It eliminates information blocking risk from the first day it goes live.
FHIR R4 and Interoperability Standards
HL7 FHIR R4 is the current standard for healthcare data exchange. It defines how patient data is structured and transmitted between systems.
SMART on FHIR extends this standard by allowing third-party clinical applications to securely connect to your EHR. This enables a growing ecosystem of specialized tools without requiring custom integrations for each one.
ONC certification under the 21st Century Cures Act requires EHR systems to support FHIR R4 APIs for patient data access. Systems built without this capability cannot achieve ONC certification.
TEFCA and the National Network
The Trusted Exchange Framework and Common Agreement establishes the national infrastructure for health information exchange. Participating Qualified Health Information Networks connect providers across the country.
Healthcare organizations joining TEFCA-connected networks need EHR systems capable of bidirectional data exchange. This is not optional for organizations participating in value-based care contracts.
EHR Software Development Cost Pricing Tiers From MVP to Enterprise
EHR software development cost ranges from $150,000 for a basic MVP to over $2 million for a full enterprise system. Where you land depends on scope, integrations, compliance requirements, and your development partner’s location and experience.
Here is a transparent breakdown across four tiers.
| Tier | What Is Included | Timeline | Cost Range | Best For |
|---|---|---|---|---|
| MVP / Pilot | Core patient records, basic scheduling, one integration, HIPAA baseline | 3 to 5 months | $150K to $350K | Startups, pilot programs, funding rounds |
| Mid-Market | Full clinical modules, 3 to 5 integrations, patient portal, RCM basics | 6 to 10 months | $400K to $850K | Regional clinics, specialty practices, 50 to 500 providers |
| Enterprise | Multi-department system, AI modules, full interoperability, custom reporting | 10 to 18 months | $900K to $2M+ | Hospital systems, multi-state networks, IDNs |
| EHR Modernization | Legacy migration, re-architecture, new UI layer on existing data | 4 to 9 months | $200K to $600K | Organizations replacing aging platforms |
What Drives Cost Up or Down?
- Integration points: each third-party system adds $20K to $80K in development cost
- Specialty modules: mental health or oncology features add 20 to 35 percent to base cost
- AI features: ambient documentation and predictive analytics add $80K to $250K depending on scope
- ONC certification testing: adds $30K to $100K to the overall project budget
- Development location: onshore US teams cost $150 to $250 per hour; offshore teams cost $40 to $90 per hour
The Hidden Cost of Not Building Custom
Epic licensing for a 200-provider organization averages $2.5 million in year one. Annual maintenance and renewal runs $400K to $800K per year after that.
A custom EHR built at the mid-market tier costs $400K to $850K upfront. There are no per-provider licensing fees. Total five-year cost typically lands between $800K and $1.5 million including ongoing support.
Over five years, most organizations find custom development 40 to 60 percent cheaper than enterprise EHR licensing.
The EHR Development Process — SoftProdigy ClinicalFirst Method
EHR development fails when it starts with technology decisions instead of clinical reality. The SP ClinicalFirst Method reverses that sequence.
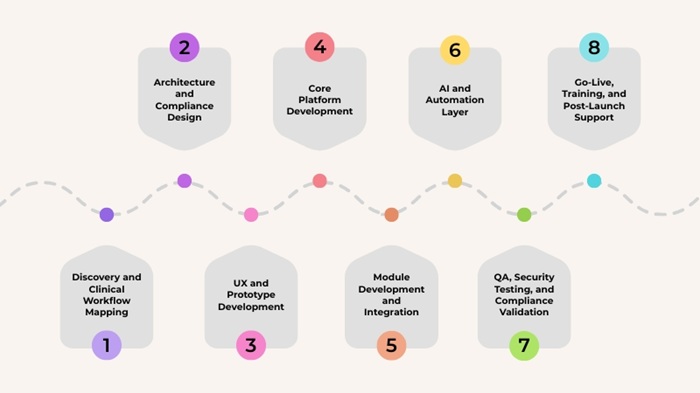
We start with the clinician’s day. Then we design the system around it. Here is how the process works across eight stages.
- Discovery and Clinical Workflow Mapping: We spend the first two to four weeks inside your clinical environment. We observe actual workflows, interview providers, and map every data touchpoint. This stage produces a Clinical Reality Document that drives every downstream decision.
- Architecture and Compliance Design: Our team designs the system architecture with HIPAA, FHIR R4, and ONC requirements embedded from day one. We define the integration map, data model, and security framework before writing any code.
- UX and Prototype Development: We build clickable prototypes of core clinical workflows. Physicians and nurses interact with these before development begins. This stage catches interface problems before they become expensive fixes.
- Core Platform Development: Our engineers build the foundation. Patient records, authentication, role-based access controls, audit trails, and the core API layer. This takes six to ten weeks depending on scope.
- Module Development and Integration: Clinical modules are built in parallel sprints. Lab, imaging, medication, and specialty modules are developed and tested against your actual workflows. Third-party integrations are built and validated during this stage.
- AI and Automation Layer: For organizations including ambient documentation or predictive analytics, this stage integrates LLM-powered clinical tools and machine learning models. AI components are validated for clinical accuracy before deployment.
- QA, Security Testing, and Compliance Validation: Every component goes through functional, integration, and penetration testing. ONC certification testing is conducted if required. Compliance documentation is produced at this stage.
- Go-Live, Training, and Post-Launch Support: We manage a phased go-live to minimize disruption. Provider training is delivered in clinical context, not classroom settings. Our team provides 90-day post-launch support with defined response times.
How Ambient Documentation and Predictive Analytics Are Changing Clinical Software
AI in EHR is no longer a future capability. It is a clinical tool delivering real results today. Here is what AI-powered EHR development actually delivers in 2026.
What Is Ambient Clinical Documentation?
Ambient documentation listens to a physician-patient encounter in real time. It uses large language models to convert that conversation into a structured clinical note. The physician reviews and approves. Documentation time drops from 15 to 20 minutes per encounter to under three minutes.
Microsoft DAX Copilot reported in 2024 that physicians using ambient documentation saved an average of 5 hours per week on administrative work. That is 260 hours per year per physician. A custom EHR embeds ambient documentation directly into the clinical workflow. The physician does not switch tools. The note appears inside the encounter automatically.
How Does an AI Medical Scribe Work?
An AI scribe transcribes clinical conversations and populates structured fields in the EHR. Unlike ambient documentation, which produces a free-text note, a scribe fills specific data fields directly.
Drug allergies, vitals, chief complaint, and assessment fields are populated automatically. ICD-10 codes are suggested based on encounter content. Billing documentation is generated as part of the same workflow.
Predictive Analytics in a Clinical EHR
Machine learning models embedded in an EHR can flag patients at risk of readmission, sepsis, or medication non-adherence before symptoms escalate. A study published in NEJM Catalyst in 2023 found that EHR-integrated predictive models reduced 30-day readmission rates by 18 percent in hospital systems that deployed them at scale.
Custom EHR development makes predictive models a native part of the clinical interface. Risk flags appear inside the patient record, not in a separate analytics dashboard.
Clinical NLP for Unstructured Data
A large portion of clinically important information lives in free-text notes. Clinical natural language processing extracts structured data from unstructured text.
This turns years of clinical notes into queryable, analyzable data. It improves population health management and supports outcomes research without requiring workflow changes from clinical staff.

EHR Integration: HL7, FHIR, Epic, Cerner, and SMART on FHIR
An EHR that cannot talk to other systems is a liability, not an asset. Interoperability is the technical backbone of modern clinical care.
Here are the standards and integration points every EHR development team must address.
HL7 v2 and v3
HL7 v2 is the legacy standard. It handles messaging between clinical systems using a pipe-delimited text format. Most labs, pharmacies and legacy hospital systems still communicate in HL7 v2. Your custom EHR must support HL7 v2 message types including ADT for admissions and transfers, ORU for lab results, and ORM for order management. Without this, you cannot connect to existing clinical infrastructure.
FHIR R4
FHIR R4 is the current standard for healthcare data exchange. It uses RESTful APIs and JSON or XML formatting. Indeed, FHIR is faster and far easier to implement than HL7 v2.
ONC certification requires FHIR R4 APIs. The 2024 Information Blocking Rule requires FHIR-based data sharing. Any EHR built without FHIR R4 is non-compliant by design.
SMART on FHIR
SMART on FHIR is an authorization framework that allows third-party applications to securely connect to your EHR’s FHIR APIs. Think of it as OAuth for clinical apps.
This framework allows specialty tools, patient-facing apps, and analytics platforms to connect to your EHR without custom integration work for each one. It is the architecture that makes a modular EHR ecosystem possible.
Epic and Cerner Integration
Many organizations have departments or partner facilities running Epic or Cerner. Your custom EHR must exchange data with these platforms reliably.
Epic’s FHIR APIs are certified and available for integration. Cerner’s Millennium platform supports FHIR R4 through its HealtheIntent data platform. Soft Prodigy has built bidirectional integrations with both platforms for existing healthcare clients.
Apple Health Records and Patient-Facing APIs
The 21st Century Cures Act requires EHR systems to provide patients with API-based access to their health records. Apple Health Records pulls patient data from connected EHRs using FHIR.
Organizations that do not support patient-facing APIs are non-compliant with the patient access rule. A custom EHR built on FHIR R4 satisfies this requirement by default.
Wrapping Up,
EHR software development is not a technology purchase. It is a clinical transformation decision.
The organizations that get it right start with a clear picture of their clinical workflows. They choose a development partner with real healthcare experience. They build for compliance from the first line of code, not as an afterthought.
Soft Prodigy has spent 20 years building technology for regulated industries. The next step does not have to be a commitment. It can be a conversation with us!










